Managing 1,000+ SOPs: What Enterprise Healthcare Policy Management Really Looks Like
When your health system maintains thousands of policies across dozens of facilities, systemic limitations and legacy infrastructure, rather than human error, drive the inefficiency. Here's what scale-ready policy management actually requires.
When a 16-hospital health system attempted to standardize policies across its facilities, the pharmacy department alone discovered 1,170 distinct documents requiring review: policies, SOPs, work instructions, and procedures scattered across facility libraries that had never been coordinated. That's just pharmacy. Multiply across nursing, administration, quality, compliance, facilities, and every other department, and enterprise health systems routinely maintain thousands of policy documents without a unified architecture.
The pharmacy standardization project consolidated those 1,170 documents down to 72 shared policies, eliminating 751 redundant or outdated documents in the process. The active consolidation took 22 weeks of dedicated meetings. And that was one department in one division.
This case highlights the predictable result of how healthcare documentation grows at scale. Every merger adds documentation. Every department maintains its own procedures. Every facility develops local practices that get written down (or don't). Nobody is in charge of the whole picture because the whole picture doesn't fit in anyone's job description.
At a certain point, call it the 500-policy threshold, or the third acquired hospital, or the moment a surveyor asks for a document and three people produce three different versions, the challenge shifts from individual retrieval to ecosystem management, exceeding human capacity..
The Scale Problem: Why Enterprise Is Different
Small practices and single hospitals have policy management challenges. But enterprise health systems face qualitatively different problems that require different solutions.
The Math of Complexity
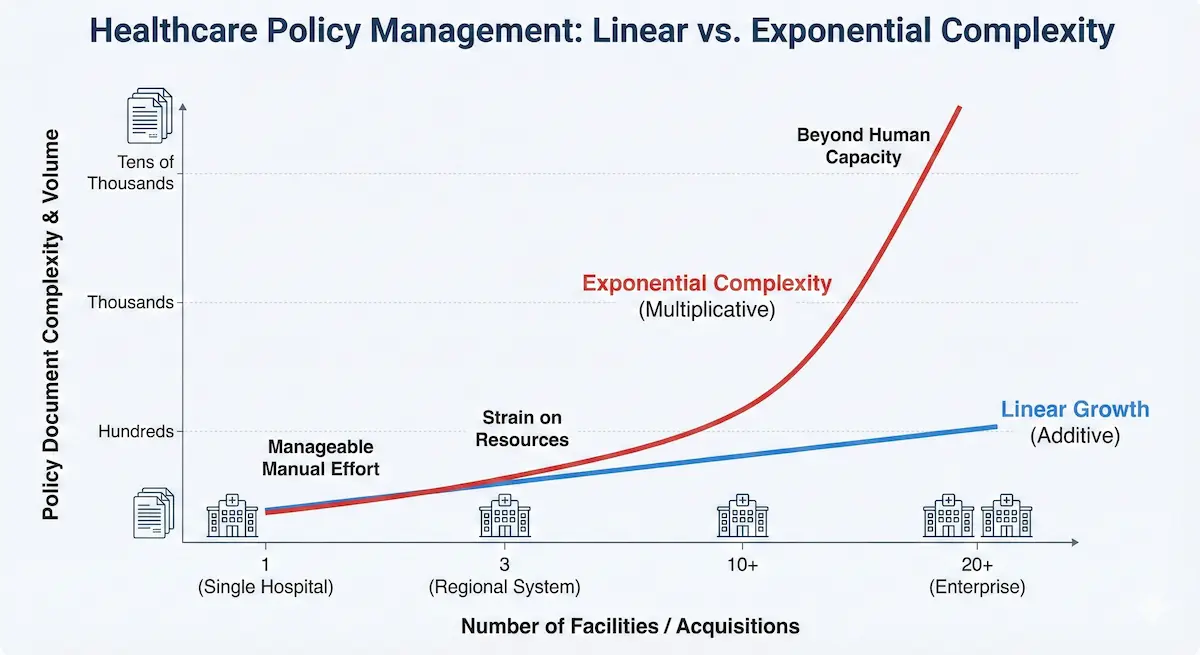
A standalone hospital might maintain 300-500 active policies. Manageable with discipline and dedicated staff.
But complexity scales exponentially rather than linearly. As we saw with the 16-hospital pharmacy example, a system doesn't just end up with 16 sets of policies; they end up with thousands of documents that overlap, contradict, or duplicate each other in ways nobody has mapped.
Extrapolate that pharmacy data across nursing, administration, quality, and compliance. Enterprise organizations are routinely managing 5,000+ distinct policy documents without a unified architecture. Every new facility adds potential contradictions with every existing policy.
The Post-Merger Documentation Hangover
Healthcare consolidation has accelerated dramatically. Each acquisition brings:
- Inherited documentation: The acquired facility's entire policy library, with its own naming conventions, folder structures, and approval workflows
- Regulatory baggage: Different state requirements if crossing state lines, different accreditation histories, different survey findings that shaped their policies
- Cultural practices: The way things were done there, documented or not, which staff expect to continue
- Technical debt: Policies referencing systems, roles, and processes that no longer exist post-merger
Most integration plans optimistically allocate 12-18 months for policy harmonization. Most organizations discover they're still reconciling documentation years later. Meanwhile, staff from different legacy organizations follow different procedures for identical situations, creating variation that's invisible until something goes wrong.
The Department Silo Problem

Even without mergers, enterprise organizations develop internal contradictions organically.
ConvergePoint's analysis of healthcare policy management challenges identified a pattern that will sound familiar: departments update their own policies independently, without visibility into related policies maintained by other departments. The nursing policy says one thing about medication administration timing. The pharmacy policy says another. The quality improvement policy references yet another standard.
Each department believes its policy is authoritative for its domain. Nobody owns the seams between domains. The contradictions accumulate until an audit finding or patient safety incident surfaces them.
The Four Pain Points That Compound at Scale
1. Policy Lookup Becomes Impossible
At a single facility, finding a policy is frustrating but eventually successful. You know the nursing educator who keeps the good copies. You know the folder structure because you've been clicking through it for years.
At enterprise scale, that local knowledge doesn't transfer. A nurse floating to a different facility struggles to locate protocols because the folder structure is different. A new hire at the corporate office can't locate the system-wide policy because it's buried in a department folder. An auditor asks for a policy and three facilities produce three documents with the same name but different content.
The AllNurses forums document the ground-level experience:
Nobody seems to know how to find most policies.
When you really want a policy to guide practice, there is none.
The core issue is retrieval, not existence. From leadership’s perspective policies exist, but operational barriers render them inaccessible.
Research from BMJ Quality & Safety quantifies the impact: 16-34% of clinical shift time is preventable waste, much of it spent searching for information, equipment, or people. At enterprise scale with thousands of policies across dozens of locations, the search problem becomes exponentially worse.
2. Conflicting Policies Create Real Risk
When a health system maintains multiple versions of policies for the same topic, staff follow whichever version they can find, or whichever their preceptor taught them, or whichever makes sense given the equipment available on their unit.
The operational consequences are tangible and documented. PSQH's analysis of healthcare policy management confirms these policy inconsistencies directly contribute to:
- Patient safety incidents: Staff following different procedures for the same clinical situation
- Compliance violations: Different facilities interpreting regulations differently
- Liability exposure: Unable to demonstrate consistent standard of care when incidents occur
The challenge is that contradictions are invisible until they cause problems. Nobody reviews all 2,000+ policies looking for conflicts. The pharmacy department doesn't read nursing policies. The acquired facility's documentation sits in a separate system that the legacy organization never fully integrated.
Without proactive detection mechanisms, organizations discover contradictions the hard way: through audit findings, patient complaints, or worse.
3. Audit Preparation Becomes a Crisis
Joint Commission surveys, CMS reviews, state inspections—regulatory bodies expect organizations to produce current, consistent documentation on demand.
At enterprise scale, this expectation collides with reality.
Joint Commission survey guidance emphasizes that surveyors assess both the existence of policies and staff's ability to access them. A policy that exists but can't be found is operationally equivalent to a policy that doesn't exist.
The pre-audit scramble is familiar to anyone who's experienced it:
- Surveyor requests policy on Topic X
- Staff search shared drives, find multiple versions
- Leadership debates which version is "official"
- Someone produces a document; nobody is confident it's current
- Surveyor notes the retrieval difficulty as a finding
Federal oversight of accrediting organizations has increased scrutiny on exactly these documentation practices. Organizations can't rely on institutional knowledge to navigate audits when institutional knowledge doesn't scale across facilities.
4. Vendor and Operational Documentation Multiplies Silently
Clinical policies get attention. The less glamorous documentation like vendor contracts, supply specifications, equipment maintenance schedules, formulary agreements, often doesn't.
Yet this operational documentation creates its own scale problems. Research on healthcare contract management found that healthcare organizations struggle to maintain visibility into contract terms, renewal dates, and pricing across vendors. Finance has equipment contracts. Pharmacy has wholesaler agreements. Procurement has supplier specs. Facilities has maintenance contracts.
When someone needs to verify a contracted price or check equipment warranty status, they email multiple departments and wait. The information exists; accessing it requires knowing who owns it and hoping they respond.
At enterprise scale with hundreds of vendor relationships across multiple facilities, this scattered documentation creates operational friction that's hard to measure but constantly present.
Why Traditional Approaches Fail at Scale
Understanding why the usual solutions don't work at enterprise scale helps clarify what's actually required.
Shared Drives Don't Scale
The shared drive model assumes that folder organization can provide findability. This works when one person designs the structure and a small team uses it consistently.
At enterprise scale, you have dozens of people creating folders, each with their own logic. You have facilities with different folder structures that were never harmonized. You have employees who left years ago whose folders contain critical documents that nobody knows exist.
Relying on shared drive navigation requires knowing where to look. At scale, nobody knows where to look because "where" is different for every facility, department, and legacy system.
Keyword Search Doesn't Scale
Search seems like the solution to folder navigation. Type what you want, find it.
But as we've explored in our analysis of folder hierarchies vs. natural language search, at scale, keyword search breaks down. A search for "medication administration" across an enterprise document repository returns hundreds of results: policy documents, training materials, committee meeting notes, regulatory summaries, and quality improvement reports from multiple facilities, multiple years, and multiple superseded versions.
Staff don't have time to review 200 search results to find the one authoritative document. They give up, ask a colleague, or follow whatever procedure they learned during training.
Policy Management Software Helps, But Doesn't Solve
Traditional policy management platforms provide version control, approval workflows, and better organization than shared drives. This is genuinely useful.
But most policy management tools don't solve:
- Cross-document contradiction detection: They manage individual policies well but don't identify when Policy A conflicts with Policy B
- Natural language access: Staff still need to know what they're looking for and navigate to it
- Operational documentation: They're designed for formal policies, not the broader knowledge ecosystem of contracts, specifications, and procedures
At enterprise scale, the gap between "policies are managed" and "staff can find answers" remains significant.
What Scale-Ready Policy Management Actually Requires
Based on the failure patterns above, enterprise healthcare organizations need solutions that address scale-specific challenges.
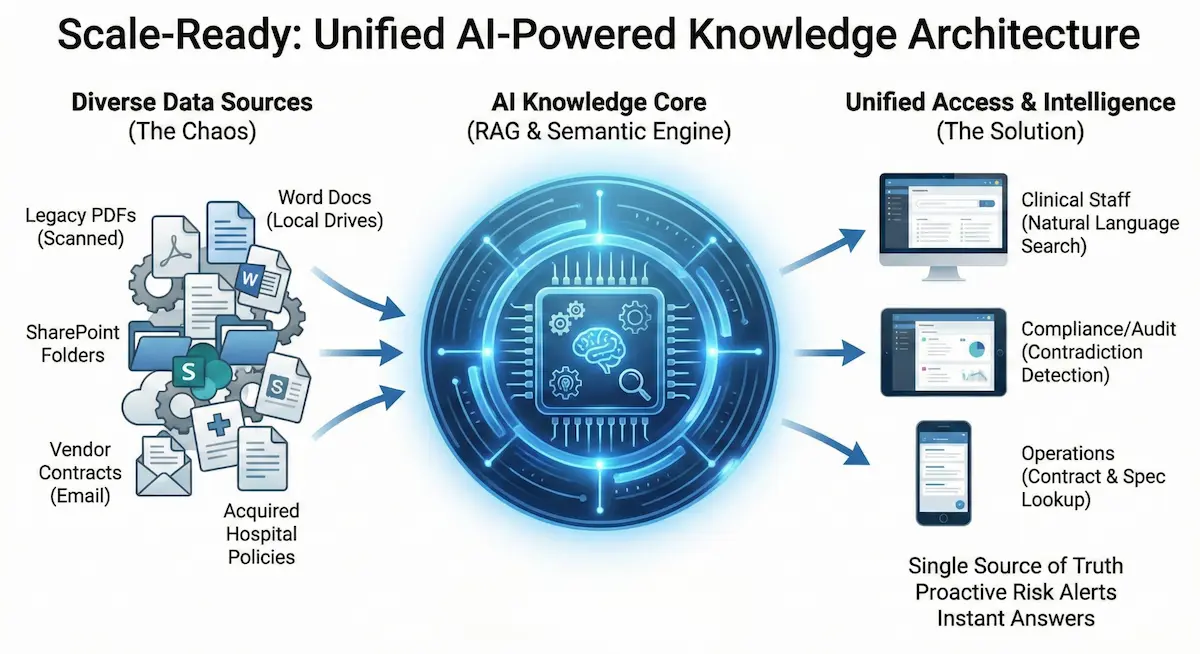
Unified Repository with Universal Access
All documentation—clinical policies, operational procedures, vendor contracts, equipment manuals—must be accessible from a single interface. Not consolidated into one physical location necessarily, but federated such that a single search covers everything.
This requires integrating legacy systems, acquired facility documentation, and department-specific repositories into a coherent whole. Technical integration is hard. Governance (who owns what, who can update what) is harder.
Natural Language Retrieval
Staff need to ask questions, not navigate hierarchies or guess keywords.
"What's our policy on family presence during resuscitation?" should return the relevant policy, not a list of documents containing those words that staff must manually filter.
This is the promise of semantic search and RAG-based systems: understanding the intent behind queries rather than just matching text strings.
Automated Contradiction Detection
At scale, manual review of all policy pairs for conflicts is impossible. Organizations need systems that can analyze the entire documentation corpus and surface:
- Direct contradictions (Policy A says 24 hours; Policy B says 48 hours)
- Implicit conflicts (two procedures that can't both be followed simultaneously)
- Outdated references (policies citing former employees, discontinued systems, superseded regulations)
- Gaps (processes referenced but never documented)
This capability is emerging in AI-powered knowledge management systems. Advanced RAG platforms with autonomous agents can perform this analysis automatically, flagging issues before auditors or patient safety incidents surface them.
Version Control with Clear Supersession
When documents are updated, the old versions must be clearly marked as superseded, not just renamed or moved to an archive folder. Staff who somehow find an old version need clear signals that it's no longer authoritative.
At enterprise scale, this requires automated version management that doesn't depend on individual document owners remembering to archive old versions properly.
Role-Based Access at Scale
Different users need access to different documents. Facility-specific policies should be accessible to staff at that facility. System-wide policies should be universally available. Sensitive operational documents (contracts, personnel policies) require restricted access.
Enterprise identity management integration becomes essential—single sign-on tied to role-based permissions that don't require manual maintenance as staff move between facilities or change roles.
The AI Opportunity: Why This Problem Is Different Now
The capabilities described above have been theoretically possible for years. Implementation at scale has been prohibitively complex and expensive.
Recent advances in AI change the equation:
Document parsing at scale: Modern AI systems can ingest PDFs (including scanned documents), Word files, spreadsheets, and other formats without manual preprocessing. An enterprise health system can upload its entire documentation library and have it searchable within days rather than months.
Semantic understanding: Natural language processing now handles clinical vocabulary, synonyms, and contextual meaning well enough that "Can an RN remove a chest tube?" correctly retrieves scope-of-practice documentation even when those exact words don't appear.
Contradiction detection: AI agents can systematically compare documents across an enterprise corpus, identifying conflicts that no human reviewer would have time to find manually.
Continuous maintenance: Unlike one-time cleanup projects, AI systems can monitor for new contradictions as documentation evolves, flagging issues as they emerge rather than after they've caused problems.
This is where the shift from "policy management software" to "knowledge management infrastructure" becomes meaningful. Beyond simple organization, the strategic imperative is ensuring institutional knowledge remains accurate, consistent, and accessible as organizations grow.
Evaluating Solutions: What to Ask Vendors
For enterprise healthcare organizations evaluating policy management modernization, the right questions reveal whether solutions actually address scale challenges:
Document Handling
- How does the system handle scanned PDFs and legacy documents from acquired facilities?
- Can it process our existing documentation without manual reformatting?
- How quickly can we ingest and search thousands of documents?
Retrieval Quality
- Can staff ask natural language questions and get direct answers?
- Does every answer cite specific documents and sections for verification?
- How does the system handle queries that span multiple policies?
Contradiction Management
- Can the system identify conflicts between policies automatically?
- Does it flag outdated references (former employees, discontinued systems)?
- How are detected issues surfaced to documentation owners for resolution?
Scale and Security
- How does the system handle multiple facilities with different policy sets?
- Can it integrate with enterprise identity management for role-based access?
- Where does data reside, and does the vendor support BAA requirements?
Maintenance Burden
- How are policy updates reflected in the system?
- Does it require manual indexing or tagging, or is processing automatic?
- What ongoing administrative overhead does the system require?
The Strategic View: Knowledge as Infrastructure
Healthcare has invested heavily in transactional systems: EHRs that capture what happened to patients, revenue cycle systems that track billing, supply chain systems that monitor inventory.
The systems that guide how staff should do their work have received far less investment. Policies, procedures, protocols, and operational knowledge remain fragmented across shared drives, legacy intranets, and institutional memory that walks out the door every time an experienced employee leaves.
At enterprise scale, this gap becomes strategic risk. Organizations can't demonstrate consistent standards of care. Audits become crises. Post-merger integration stalls on documentation reconciliation. Staff waste hours daily searching for information that should be instantly accessible.
The organizations that treat knowledge management as infrastructure, investing in systems that scale, integrating documentation across facilities, implementing proactive quality management, will operate more efficiently, navigate audits more confidently, and onboard staff more effectively.
The organizations that continue treating policy management as an administrative afterthought will continue experiencing the same frustrations, just at larger scale with higher stakes.
Getting Started: Practical Next Steps
For clinical informatics and quality leadership evaluating the path forward:
1. Audit your current state honestly
- How many distinct policy repositories exist across your organization?
- Can staff at any facility find system-wide policies quickly?
- When was the last time someone systematically reviewed documentation for contradictions?
2. Quantify the pain
- How long does it take to locate specific policies during audits?
- What percentage of new hire orientation time addresses "how to find things"?
- How many survey findings in recent years related to documentation access?
3. Define success criteria
- What retrieval time is acceptable for policy questions?
- What level of contradiction detection would meaningfully reduce risk?
- What integration requirements are non-negotiable (SSO, mobile access, legacy system connectivity)?
4. Evaluate solutions against scale requirements
Not all policy management tools address enterprise challenges. Test prospective systems with your actual documentation: messy scanned PDFs, contradictory policies from acquired facilities, the full complexity of your real environment.
The technology to manage policy documentation at enterprise scale exists today. The question is whether organizations will modernize proactively or continue working around systems that stopped scaling years ago.
For a deeper technical exploration of how AI-powered knowledge management works in healthcare settings, see our complete guide to RAG-based clinical knowledge management.
Frequently Asked Questions
Large health systems commonly maintain thousands of active policies across clinical, operational, administrative, and compliance domains. One 16-hospital system found 1,170 documents in the pharmacy department alone requiring review, and that's just one department. Across all departments, enterprise systems routinely manage 2,000-5,000+ distinct policy documents.
Scale creates exponential complexity. Each facility adds its own policies. Departments update documents independently. Mergers and acquisitions layer additional documentation. Without centralized architecture, organizations end up with contradictory policies, version chaos, and staff who can't find authoritative guidance.
Conflicting policies develop when departments update their own documents without coordination. Nursing specifies one timeframe while pharmacy specifies another for the same process. Merged facilities maintain separate protocols. Without automated detection, these contradictions go unnoticed until audits or patient safety incidents surface them.
Joint Commission and CMS surveyors assess whether staff can quickly retrieve current policies, whether documentation is consistent across departments, and whether version control prevents outdated guidance from remaining in circulation. Scattered policies and retrieval delays are common survey findings.
Scale-ready systems require centralized repositories with universal search, automated contradiction detection across documents, version control with clear supersession chains, role-based access controls, and ideally AI-powered retrieval that understands natural language queries rather than just keywords.